
- Acute Kidney Injury (AKI) is an acute worsening of kidney function
- Globally, AKI is common in patients who are hospitalized for various reasons
- The incidence rates of AKI in hospitalized patients vary between 14.7-31.5%
- The ISN 0by25 Global Snapshot study showed that 80% of AKI in lower and lower middle-income countries (LLMICs) was community-acquired
- Dehydration and hypotension were recorded as causes in 46% and 38% of patients from LLMICs
- Mortality was 12% at one week after AKI in LLMICs
- A further ISN 0by25 study that explored recognition and management of AKI in low resource settings showed mortality rate of 15.8% after AKI
- Majority were young or previously healthy with no major co-morbidities
- Up to one fourth of patients with community acquired AKI may not recover completely and progress to chronic kidney disease (CKD)
- The impact, especially of severe forms of AKI, can be devastating.
- AKI, even milder form, is associated with adverse long-term outcomes such as proteinuria, hypertension or chronic kidney disease (CKD)
- CKD is associated with a significant increased risk of cardiovascular disease and mortality
- There is immense scope for primary or secondary prevention of AKI, particularly at lower levels of healthcare delivery systems and community
- The objective of this toolkit is to provide basic information and assist development of local context specific workflows which can be adapted for implementation by users
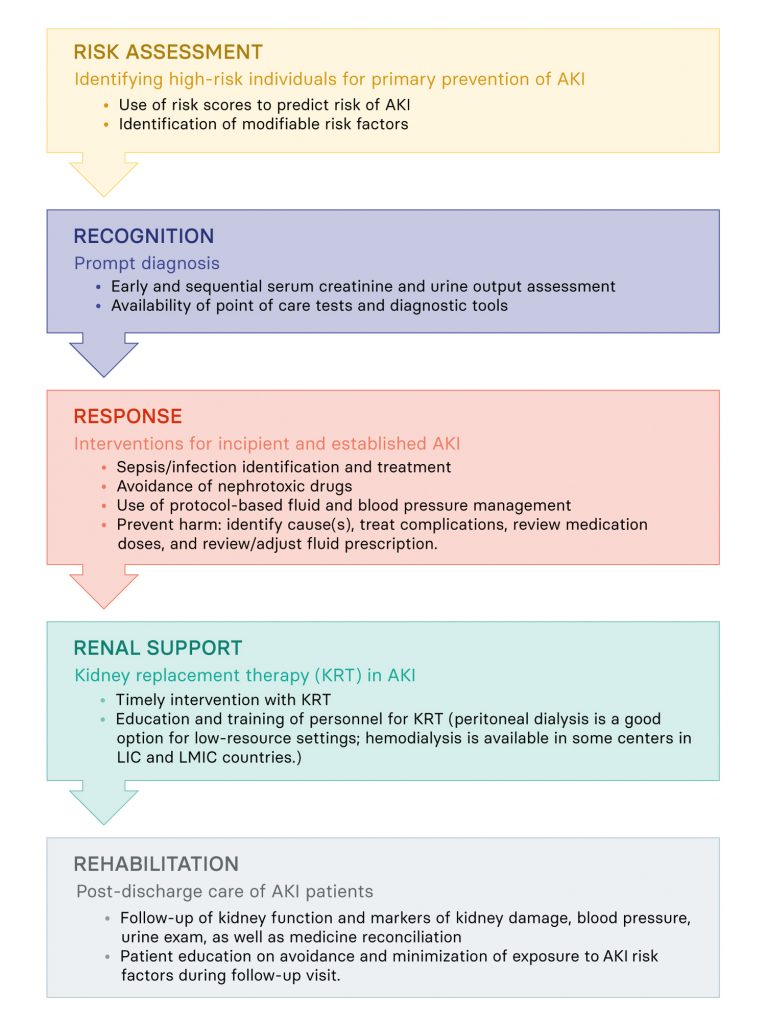
- Broadly, it is based on the 5R approach:
The objective of this toolkit is to develop and implement context specific solutions to address AKI. A quick recap of AKI in your clinical practice will help keep the context and solutions relevant. Therefore, before you start, just answer the following questions:
Download ISN AKI Toolkit ‘Before you start’ form
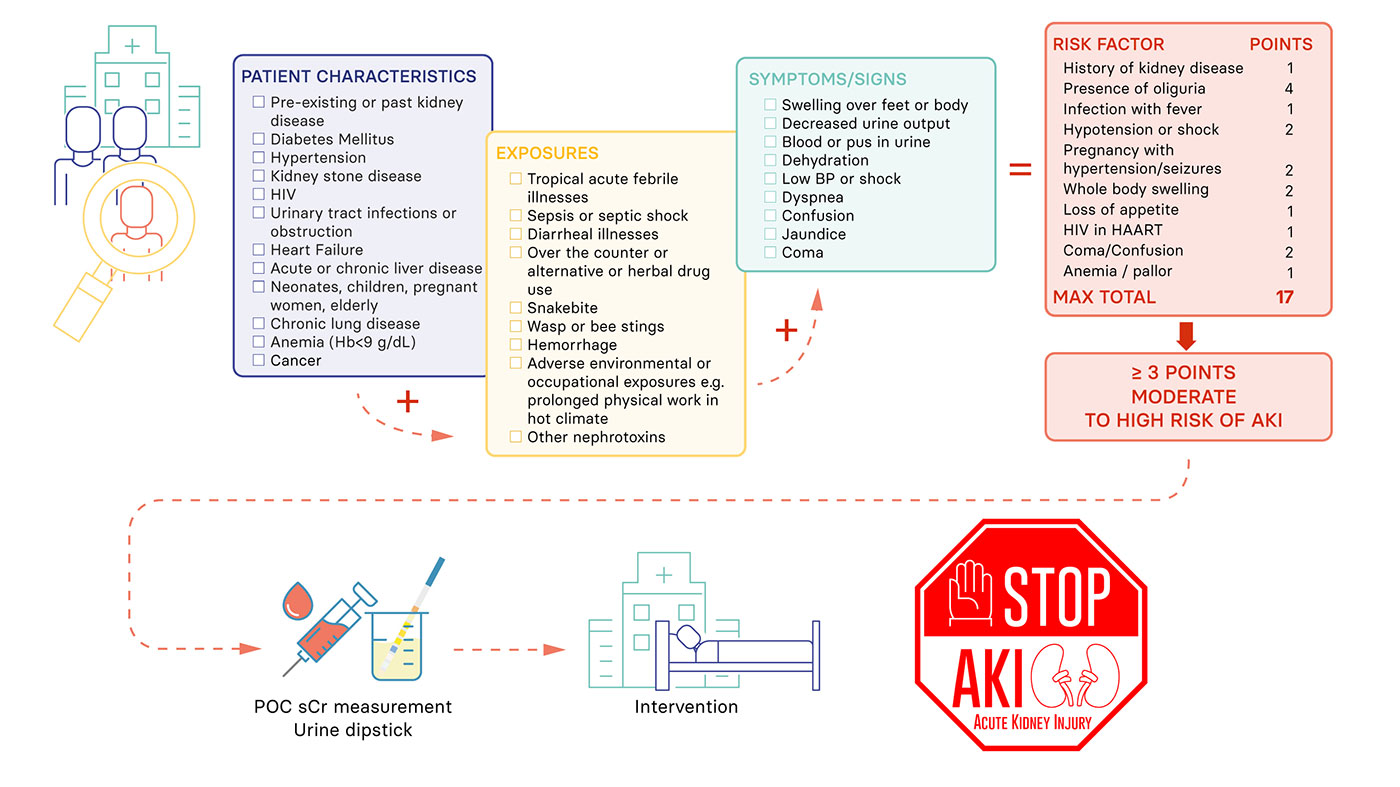
- Clinical suspicion, early recognition and management are sequential pathways for optimal AKI care
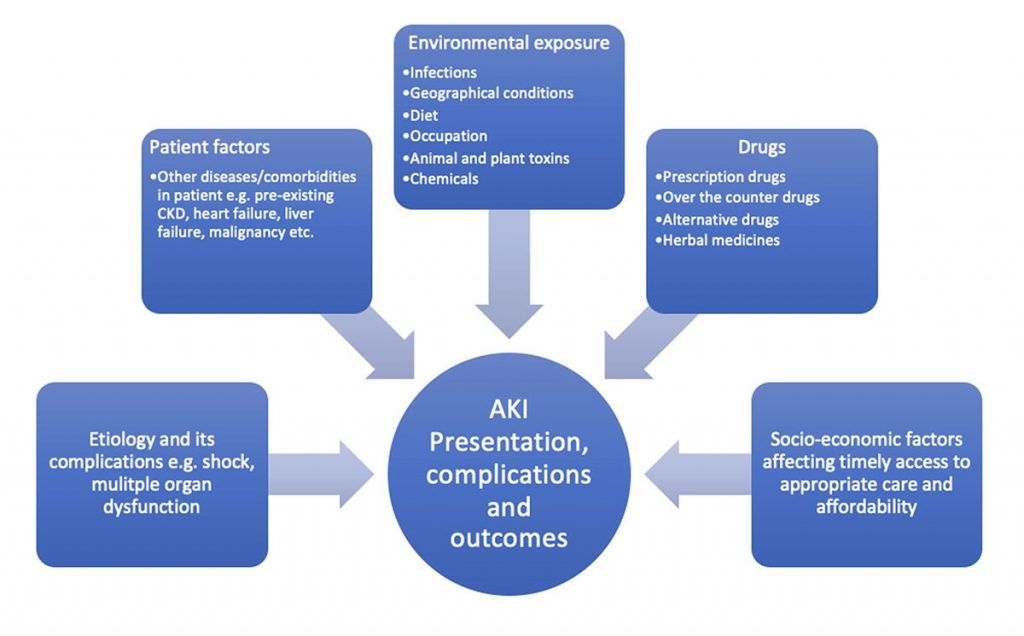
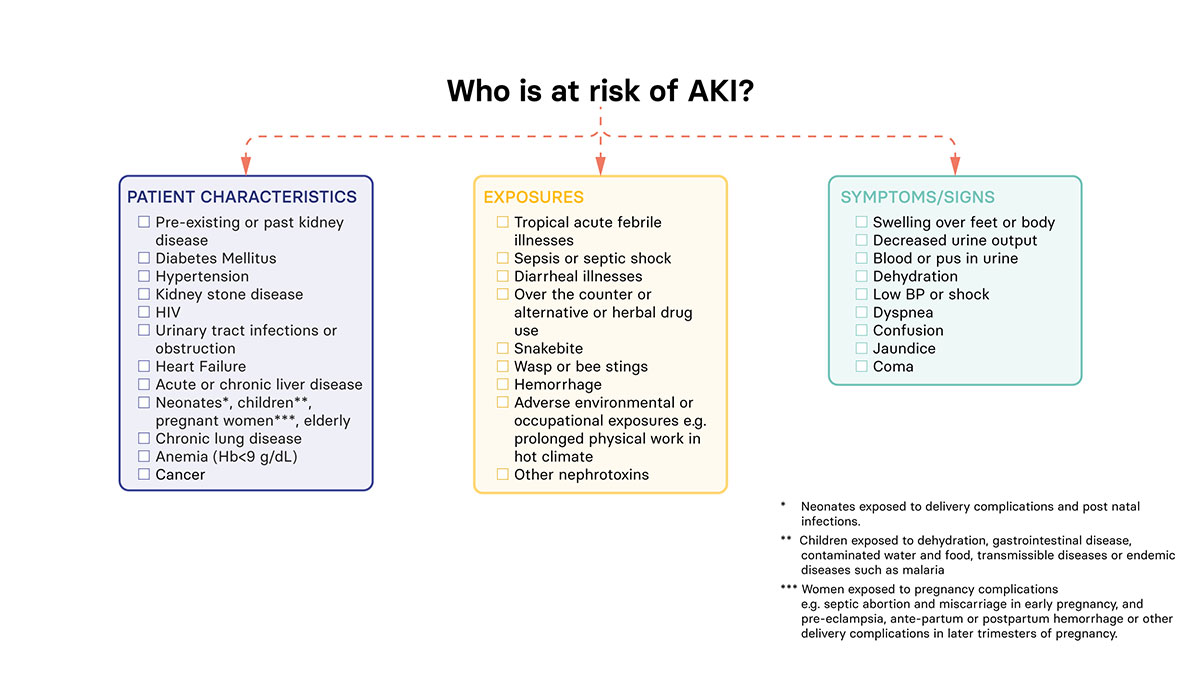
- The initial step is to identify patients with clinical presentations or other clinical features which have a high likelihood of being associated with AKI
- It is important to implement a management plan as soon as possible in any patient developing AKI to prevent further injury and reduce the risk of longer-term kidney damage
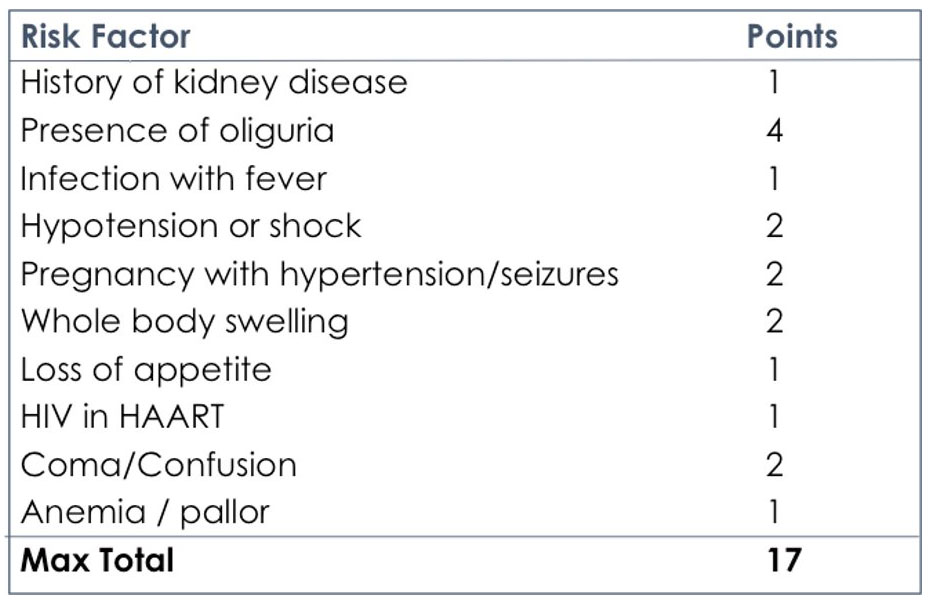 Points ≥3 can be taken as cut off to identify patients at moderate to high risk of AKI
Points ≥3 can be taken as cut off to identify patients at moderate to high risk of AKI
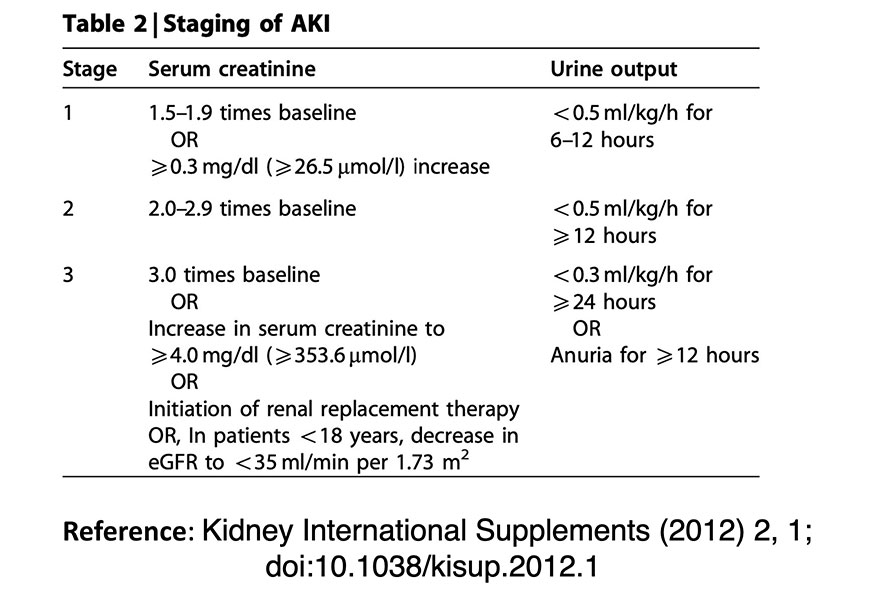
Typically, this is done by monitoring urine output and measuring serum creatinine. The current KDIGO definition of AKI is:
‘AKI is diagnosed by an absolute increase in serum Creatinine (sCr), at least 0.3 mg/dL (26.5 μmol/L) within 48 hours or by a 50% increase in sCr from baseline within 7 days, or a urine volume of less than 0.5 mL/kg/h for at least 6 hours’
However, in the absence of a baseline value, an elevated serum creatinine and appropriate clinical context is highly suggestive of AKI
KDIGO AKI classification table
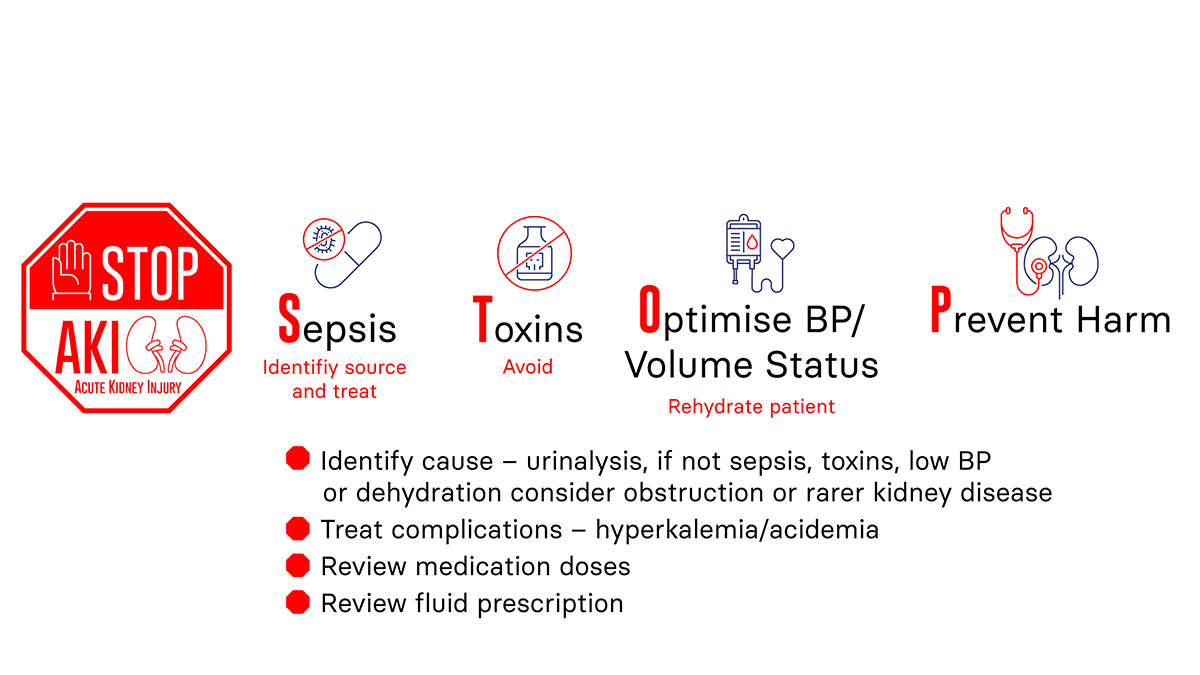
STOP AKI protocol: 4 major components
- Sepsis: Screen, treat
- Toxin: Avoid toxins
- Optimize: Blood pressure, volume status
- Prevent: Harm
- Empirical treatment based on local epidemiology of infections that are commonly associated with AKI e.g. undifferentiated acute febrile illness due to malaria, scrub typhus, dengue, etc.
- Clinical assessment and investigations (if available) to screen for other sources of infection and provide appropriate treatment
- Adjust treatment according to patient creatinine clearance/estimated glomerular filtration rate (eGFR)
- Microbial stewardship – careful review of antibiotics with cessation once sepsis treated
- Inquire/look for exposures that are commonly associated with AKI in the community e.g. snakebite, wasp/bee stings, poisonings
- Specifically, seek history of alternative or traditional or local drug intake
- Screen recent prescriptions for use of nephrotoxic drugs such as non steroidal anti-inflammatory drugs (NSAIDs), aminoglycosides, proton pump inhibitors (PPIs), herbal medicine etc.
- Collaborate with traditional healers in maintaining treatments free of toxic risk
- Withhold nephrotoxic drugs e.g. NSAIDs, aminoglycosides
- Withhold angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor antagonist (ARA-II) / angiotensin II receptor blocker (ARB)
- Withdraw herbal medicines
- Institute specific measures, if warranted e.g. anti snake venom (ASV) in case of snake bite
- Pay attention to dose modification of prescribed drugs
- For an overview of common drugs that cause Acute Interstitial Nephritis, please refer to the table in the Appendices section.
- Assess for volume status
- Symptoms and signs of volume depletion
- Equally important is clinical assessment for possible fluid overload and the need for fluid de-escalation in patients with AKI especially the ones who have decreased urine output.
- Optimize blood pressure (BP)
- Volume repletion in patients with hypotension and clinical signs of volume depletion: Target systolic BP >90 mm of Hg
- Use fluids and vasopressors (when available)
- Balanced crystalloid solutions e.g. Ringer’s lactate are preferable. However, normal saline can be used if balanced solutions are not available.
- Usually, initial resuscitation would mean 500 ml bolus over 10-15 minutes in adults as rescue therapy and smaller boluses of 100-200 ml in 10-15 minutes for optimization (ROSE protocol). In children with moderate to severe dehydration, a rapid infusion of 10-20 ml/kg may be used.
- Monitor clinical response in terms of perfusion, volume status, blood pressure and urine output
- Avoid fluid overload, close monitoring after each administration
- Stop all drugs that can lead to hypotension (e.g. diuretics, other antihypertensives)
- Volume repletion in patients with hypotension and clinical signs of volume depletion: Target systolic BP >90 mm of Hg
- Prevent volume depletion
- Identify cause of AKI
- if not sepsis or hypovolaemia consider urinary tract obstruction or rarer causes (e.g. poisonings like ethylene glycol, animal or plant toxins, herbal remedies etc.)
- Avoid nephrotoxic drugs or subsequent exposures
- Adjust medications doses
- Early referral for those patients who do not respond favourably to initial interventions, e.g.
- Persistent hypotension despite fluid resuscitation
- Persistent oliguria
- Monitor for complications to decide on timely referral to higher centre for care and/or kidney replacement therapy:
-
- Serial clinical assessments to look for
- Fluid overload
- Respiratory distress
- Worsening sensorium
- Pericarditis
- Serial evaluation of laboratory parameters (if available)
- Worsening acidosis
- Hyperkalemia
- Serial clinical assessments to look for
-
- Please consider referring a patient to a specialist if severe AKI is present (AKI stage 3) or acute-on-chronic kidney injury, if the underlying cause is not readily apparent or if there’s suspicion of an ‘intrinsic’ renal disease (for example, the presence of blood and protein in urine dip tests or indications of a multi-system disease).
Follow-up visit should include check on:
- Kidney function or damage [serum creatinine, eGFR (CKD-EPICr 2021 equation and CKiD Under 25 (U25) for patients below the age of 25), urinalysis, proteinuria] should be checked to assess for the degree of resolution of AKI, new onset of AKI or development of CKD
- Blood pressure control
- Medications: e.g. some of the medicines that may have been discontinued during the episode of AKI may need to be resumed (e.g, anti-hypertensives) or doses may have to be adjusted if patient has developed CKD or pre-existing CKD has progressed.
- Patient’s understanding of AKI and its risk factors in order to prevent future episodes
- Certain categories of patient with AKI may need earlier follow-up (within 2 to 4 weeks)
- Patients who have had severe AKI (AKI stage 3 or needed dialysis)
- Patients who have had incomplete or no recovery of kidney function at hospital discharge
- Patients with co-morbidities such as underlying CKD, heart failure, diabetes, hypertension, chronic lung disease, or on cancer treatment etc.
- Atypical clinical course or failure to recover during follow-up: Necessitate specialist referral to ascertain the cause
- May need imaging [e.g. Computed Tomography (CT) for acute cortical necrosis following post-partum AKI or snakebite related AKI] or kidney biopsy under special circumstances
Authors:
Rolando Claure-Del Granado (University of San Simón, Bolivia)
Rahul Chanchlani (McMaster University, Canada)
Robert Kalyesubula (Makekere University, Uganda)
Vivek Kumar (PGIMER, India)
Eranga Wijewickrama (University of Colombo, Sri Lanka)
Support experts:
Jorge Cerda (Albany Medical College, USA)
Etienne Macedo (UC San Diego School of Medicine, USA)
Andrew Lewington (Leeds Teaching Hospitals NHS Trust, UK)