
June 2026 Edition

Impact Factor 2025
New tools, better care: kidney research from KI/KIR
This month’s Kidney International® selection focuses on improved risk prediction, earlier prevention, and more inclusive evidence generation, reflecting broader efforts to strengthen the evidence base for kidney care.
The Kidney International Reports® collection complements this theme with studies on telehealth, artificial intelligence-supported diagnostics, and community health worker-led interventions that aim to improve access, engagement, and outcomes across diverse patient populations.

KIDNEY INTERNATIONAL ARTICLES |
Population-based estimated glomerular filtration rate distributions and associated health outcomes provide opportunities for early identification of and primary prevention of chronic kidney disease
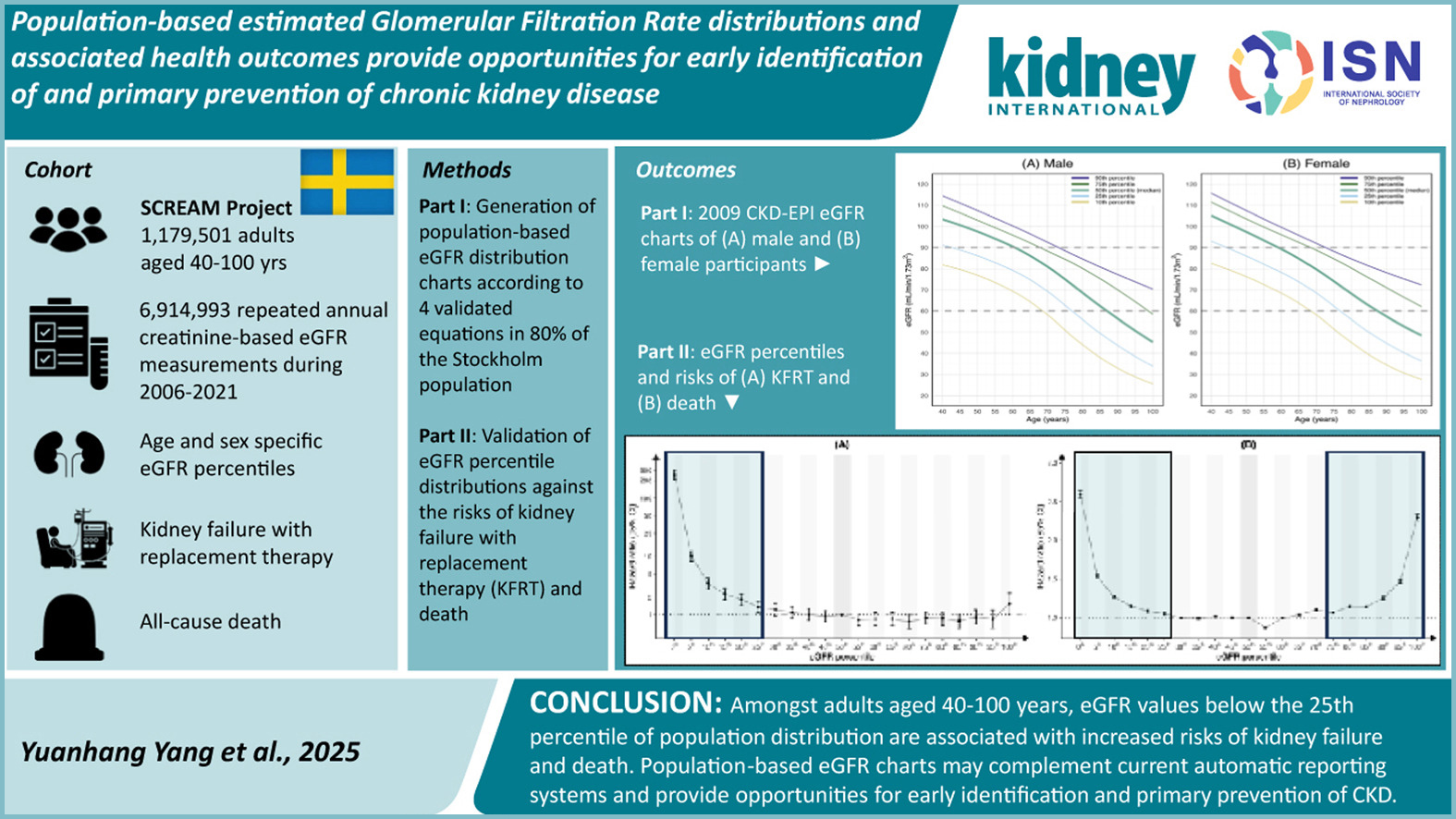
There are currently no established optimal strategies for the primary prevention of chronic kidney disease (CKD). This study aimed to characterize the distribution of estimated glomerular filtration rate (eGFR) in the general population to help identify individuals at increased risk.
Using health care data from a large, representative Swedish region between 2006 and 2021, the authors constructed age- and sex-specific eGFR distributions among adults aged 40 years and older. They found that eGFR values below the 25th percentile of the population distribution were associated with higher risks of kidney failure and death. These findings suggest that population-based eGFR distributions could complement current automated eGFR reporting and support earlier identification of individuals with CKD or at increased risk, potentially informing future primary prevention strategies.
Utilizing risk prediction models for older patients with chronic kidney disease
Older adults form a growing proportion of patients with advanced chronic kidney disease (CKD), but disease progression is often unpredictable. Many progress slowly and die from competing conditions, especially cardiovascular disease, before reaching kidney failure. This complicates dialysis planning, as preparation that is too early may cause unnecessary procedures and anxiety, while late preparation may limit options. The paper argues that eGFR alone is insufficient and that personalized risk prediction may better guide decisions between dialysis and conservative care.
The review examines prediction tools, including Kidney Failure Risk Equation (KFRE), the Grams model, the Mortality Risk Equation for Kidney disease (MREK), combined KFRE/MREK use, and KDpredict. KFRE is widely validated for kidney failure risk, but may overestimate long-term risk in older adults because it does not fully account for competing mortality. MREK estimates mortality risk, while KDpredict estimates both kidney failure and death, including in conservatively managed patients. The authors conclude that these tools should support shared decision-making alongside frailty, comorbidity, quality of life, and patient preferences.
Equity in evidence: overcoming barriers to kidney trials in low-resource settings
This article highlights a major inequity in global nephrology research: the persistent underrepresentation of low- and middle-income countries (LMICs) in kidney clinical trials, despite their substantial burden of chronic kidney disease.
The authors frame this gap as both a scientific and ethical concern, since evidence generated mainly in high-income settings may not reflect the realities of vulnerable health systems. As a result, clinicians and policymakers in LMICs often face a disconnect between guideline recommendations and feasible kidney care.
A key strength of the article is the authors’ systems-level approach, which links research inequity to workforce, infrastructure, funding, and regulatory barriers. The proposed solutions, community engagement, telehealth follow-up, and pragmatic trial designs, are particularly relevant for reducing barriers to participation.
Although some recommendations remain aspirational and require clearer operational and funding pathways, this paper is an important call for more inclusive, locally driven, and context-sensitive nephrology research.
Taking the “unknown” out of CKDu — optimizing approaches to uncover the cause(s) of epidemic-level kidney disease in low and middle-income settings: a report from the ISN’s International Consortium of CKDu Collaborators (ISN i3C)
This ISN i3C meeting report provides a valuable synthesis of chronic kidney disease of undetermined etiology (CKDu), particularly epidemic-level clusters in Central America and South Asia that disproportionately affect disadvantaged communities.
The authors identify four major exposure groups: heat stress, agrichemicals, metals/metalloids, and infections, while acknowledging that no single cause has been conclusively established. They also emphasize key barriers, including inconsistent terminology, limitations of cross-sectional studies of estimated glomerular filtration rate, and the lack of early urinary biomarkers for tubulointerstitial injury.
The report’s main contribution is reframing CKDu beyond a vague “multifactorial” model by distinguishing initiating from exacerbating factors. This distinction has important implications for future research, especially when exposures such as heat stress may worsen pre-existing subclinical disease rather than initiate it. Although implementing standardized definitions, biomarkers, and biopsy-based studies will be challenging in low-resource settings, the report offers a rigorous, timely roadmap for coordinated prospective research.
Changing paradigms of studies in kidney diseases
This meeting report summarizes an International Society of Nephrology consensus meeting focused on improving clinical research in kidney diseases. The 2-day meeting brought together 76 stakeholders from all 10 ISN regions, including clinicians, trialists, statisticians, researchers, regulators, industry representatives, and patient partners. Discussions centered on patient-reported outcome measures, alternatives to single biomarker targets, novel trial designs, and hierarchical composite end points.
The report proposes a roadmap to make nephrology trials more inclusive, patient-centered, and clinically meaningful. Key priorities include validating patient-centered outcomes, rethinking biomarkers to avoid over-reliance on single targets, promoting equity and diversity across age, sex, geographic setting, and disease severity, supporting innovation in trial design, validating meaningful composite endpoints, and strengthening collaboration through public-private partnerships and sustained long-term funding.
KIDNEY INTERNATIONAL REPORTS ARTICLES |
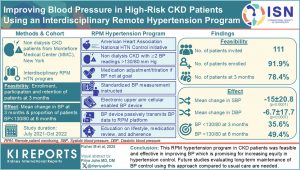
Hypertension affects more than 80% of patients with chronic kidney disease (CKD) and is among the strongest modifiable risk factors for cardiovascular disease, premature mortality, and progression to kidney failure. Despite guideline recommendations targeting blood pressure (BP) <130/80 mmHg, fewer than half of patients with CKD achieve adequate BP control, with particularly poor outcomes reported among Black and Hispanic populations.
Key barriers include limited access to frequent follow-up, therapeutic inertia, poor adherence, and reliance on office-based BP measurements. This study evaluated whether an interdisciplinary remote patient monitoring (RPM) hypertension program could improve BP control in a predominantly Black and Hispanic CKD population through home BP monitoring, telemedicine review, lifestyle education, and protocol-driven medication adjustment.
The program demonstrated feasibility and clinically meaningful improvements in BP control. Of 111 invited patients, 102 enrolled and 87 remained engaged at 3 months, with participants regularly transmitting home BP readings using cellular-enabled devices. Mean systolic BP decreased by 15.0 mmHg and diastolic BP by 6.7 mmHg within 3 months, and nearly half of participants achieved BP <130/80 mmHg by 6 months. These improvements occurred with only a modest increase in antihypertensive medication use and without serious safety concerns.
Overall, the study supports structured, remote, team-based hypertension management as a practical strategy to improve BP control and potentially reduce healthcare inequities in high-risk CKD populations.
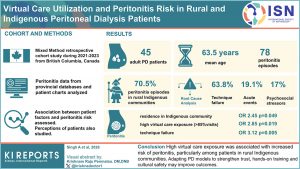
As virtual care rapidly expands in nephrology, its potential to improve access while addressing longstanding inequities in kidney care has become a growing area of interest. This study highlights the role of virtual care in addressing disparities in peritoneal dialysis (PD) outcomes among rural and Indigenous populations.
These groups face persistent challenges, including geographic isolation, limited access to specialist care, and systemic inequities that may contribute to higher peritonitis risk. The authors examine whether virtual care modalities, such as telemedicine and remote clinical support, can enhance monitoring, strengthen connection with care teams, and facilitate earlier intervention in this high-risk population.
Importantly, the findings suggest that greater virtual care exposure, particularly among Indigenous patients, may paradoxically be associated with increased peritonitis risk, potentially due to disrupted relational continuity and reduced hands-on technique assessment. These results underscore the need to rebalance virtual care strategies by prioritizing culturally safe, flexible, and community-engaged models. As hybrid systems evolve in the post-pandemic era, ensuring trust, equity, and adequate clinical oversight will be essential to optimizing outcomes in underserved PD populations.
Adaptation of navigate-kidney: A community health worker intervention for people with kidney disease
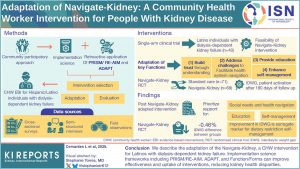
As health systems increasingly prioritize patient-centered and equitable models of care, community health worker (CHW)-led interventions have emerged as a promising strategy to bridge gaps in chronic disease management.
The adaptation of the Navigate-Kidney program represents an important step in this direction, targeting individuals with kidney disease who often face complex medical and social barriers that limit access to traditional care. This study evaluates key outcomes, including patient engagement, care coordination, healthcare utilization, and patient-reported measures such as knowledge, self-efficacy, and satisfaction with care.
The findings demonstrate that integrating CHWs into kidney care teams is both feasible and impactful, with improvements in patient navigation, helping patients identify and navigate resources for health-related social needs, and supporting culturally responsive care and sustained patient engagement.
Importantly, the adapted intervention addresses social determinants of health while enhancing patients’ confidence in managing their disease. By highlighting measurable gains in both clinical and patient-centered outcomes, this work underscores the potential of CHW-driven models to improve equity and quality in nephrology care, supporting their broader integration into routine practice.
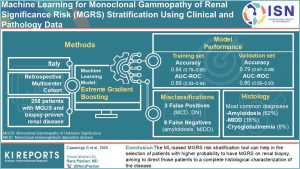
Early recognition of monoclonal gammopathies of renal significance (MGRS) is essential to guide timely treatment. However, kidney injury in patients with monoclonal gammopathy may also result from diabetes, hypertension, or primary glomerulonephritis. Although kidney biopsy remains the diagnostic gold standard, it may not be feasible in all suspected cases. This retrospective study developed a machine learning (ML) tool to support pre-biopsy risk stratification and help identify patients most likely to benefit from histologic evaluation.
The study included 258 patients with monoclonal gammopathy of undetermined significance and available kidney biopsy results. Overall, 168 patients were classified as MGRS cases and 90 as non-MGRS. MGRS was associated with female sex, more frequent Bence Jones proteinuria, and amyloidosis as the most common renal diagnosis. In the validation set, the ML model achieved an accuracy of 0.79 and an area under the receiver operating characteristic curve of 0.80.
In conclusion, this ML-based risk stratification tool may help identify patients with a higher likelihood of MGRS on kidney biopsy and support decisions regarding the need for detailed histological characterization.
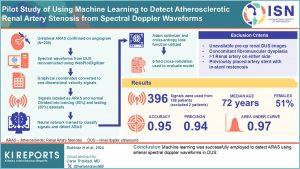 This pilot study evaluated whether machine learning can detect atherosclerotic renal artery stenosis (ARAS) using spectral Doppler waveforms obtained from renal duplex ultrasound.
This pilot study evaluated whether machine learning can detect atherosclerotic renal artery stenosis (ARAS) using spectral Doppler waveforms obtained from renal duplex ultrasound.
Patients with unilateral, angiography-confirmed ARAS who underwent renal artery stenting were retrospectively identified, and the contralateral kidney served as the control. A total of 396 Doppler signals were extracted from 198 patients, with two signals per patient: one from the ARAS kidney and one from the control kidney.
Waveform envelopes were manually traced and converted into one-dimensional velocity signals to train a one-dimensional convolutional neural network.
The model demonstrated strong diagnostic performance, with a 5-fold cross-validation accuracy of 0.94 and a Receiver Operating Characteristic Area Under the Curve (ROC AUC) of 0.98. On an unseen test set, the final model achieved an accuracy of 0.95 and a ROC AUC of 0.97. These findings support the feasibility of using a 1-dimensional CNN model to detect ARAS and assist automated diagnosis of clinically significant disease.