
December 2025 Edition

Impact Factor 2024
Key updates on IgAN & complement disorders from KI/KIR
From the efficacy and safety of felzartamab to targeting von Willebrand factor platelet interactions, in this edition, Kidney International® and Kidney International Reports® introduce new findings on IgA nephropathy and complement-mediated kidney diseases, including C3 glomerulopathy and immune complex–mediated membranoproliferative glomerulonephritis. Highlights include data-driven disease endotyping, emerging biomarkers, and updates from pivotal trials that refine risk stratification, monitoring, and targeted therapy across these complex conditions.

KIDNEY INTERNATIONAL ARTICLES |
Hierarchical clustering uncovered disease patterns and further untangled complexities in immune complex-mediated idiopathic MPGN and C3 glomerulopathy
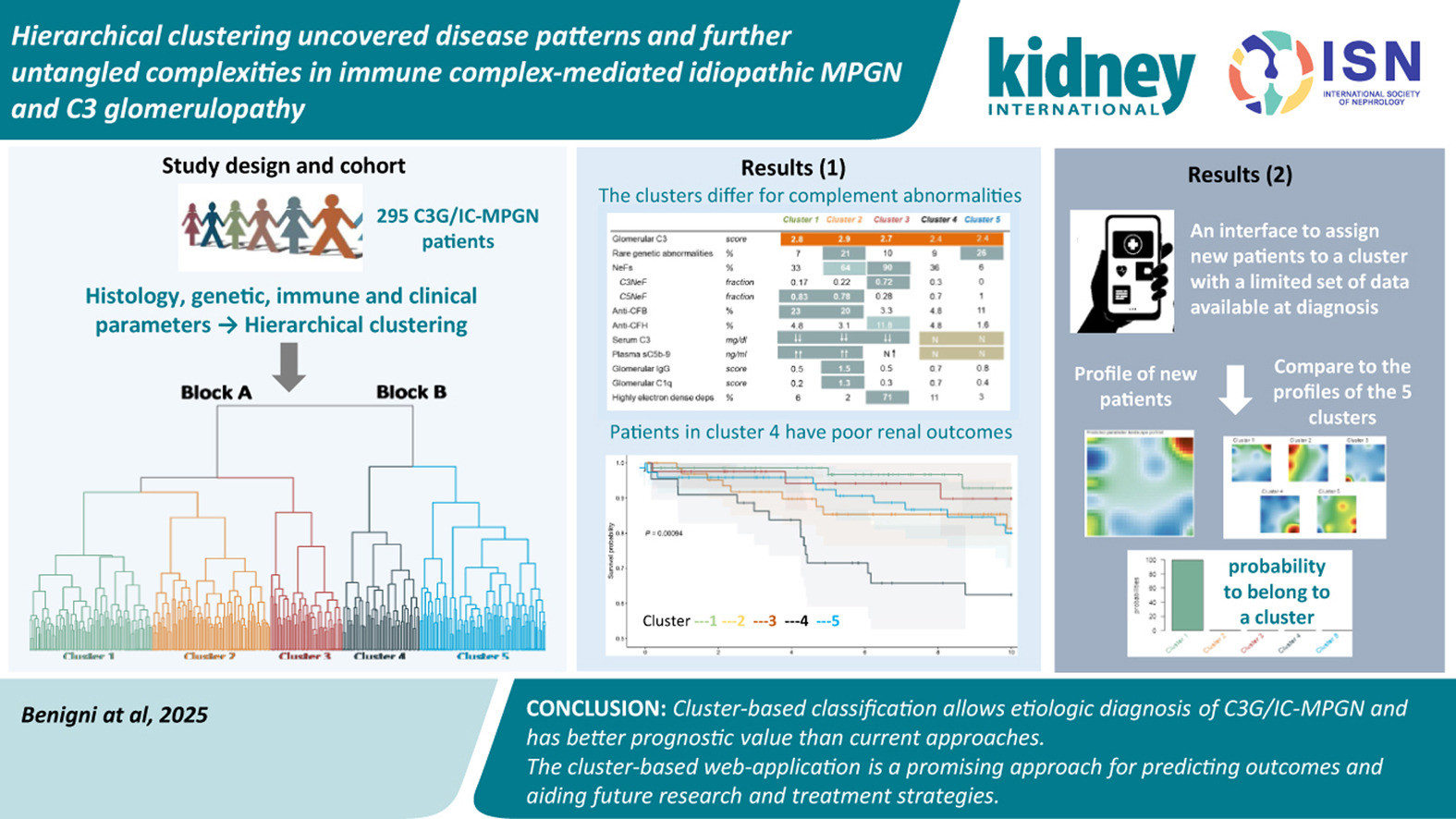
A recent cohort analysis of 295 patients with membranoproliferative glomerulonephritis (MPGN) and C3 glomerulopathy (C3G) applied hierarchical clustering to integrate phenotype with complement biology.
Five reproducible clusters emerged, each defined by distinct clinical features, degrees of complement activation, autoimmune abnormalities, and genetic variants. This cluster-based classification outperformed traditional histology in predicting kidney outcomes and post-transplant recurrence, underscoring its potential to guide risk stratification and therapeutic selection.
For clinicians, these findings support moving beyond morphology toward data-driven endotyping that aligns patients with targeted interventions. For researchers, the results highlight the need to validate clusters across diverse populations and prospectively test whether cluster-informed therapy improves outcomes. If confirmed, this approach could operationalize precision nephrology in complex glomerular diseases, linking mechanistic profiles to individualized care.
Quantifying association of early proteinuria and estimated glomerular filtration rate changes with long-term kidney failure in C3 glomerulopathy and immune-complex membranous proliferative glomerulonephritis using the United Kingdom RaDaR Registr
 Drawing on 371 patients from the UK RaDaR Registry (median follow-up 11.0 years), Masoud et al. report that 40% progressed to kidney failure and, importantly, the risk was similar between C3 glomerulopathy and immune-complex-membranous proliferative glomerulonephritis (MPGN). Baseline proteinuria did not predict failure, and early two-year estimated glomerular filtration rate slope showed only a modest association, sharpening the clinical focus on short-term proteinuria response after diagnosis.
Drawing on 371 patients from the UK RaDaR Registry (median follow-up 11.0 years), Masoud et al. report that 40% progressed to kidney failure and, importantly, the risk was similar between C3 glomerulopathy and immune-complex-membranous proliferative glomerulonephritis (MPGN). Baseline proteinuria did not predict failure, and early two-year estimated glomerular filtration rate slope showed only a modest association, sharpening the clinical focus on short-term proteinuria response after diagnosis.
Both relative (20–50%) and absolute (≥50 mg/mmol) reductions in urine protein-creatinine ratio (UPCR) within the first 12 months were linked to lower long-term risk, with the strongest signal for achieving UPCR <100 mg/mmol at 12 months (HR ~0.10, 95% CI 0.03–0.30).
Taken together, these data support early proteinuria control as a pragmatic treatment target and a candidate surrogate endpoint for trials in complement-mediated MPGN, while underscoring the need to pair optimized supportive care with timely disease-modifying strategies.
Kidney injury and colocalization of complement C3, IgA, and IgG in glomerular immune-complex deposits of patients with IgA nephropathy or IgA vasculitis with nephritis
 This retrospective biopsy study examined how complement C3 colocalizes with IgA and IgG within glomerular immune-complex deposits in IgA nephropathy (IgAN) and IgA vasculitis with nephritis (IgAVN). Greater C3–IgA colocalization is significantly associated with individual features of active glomerular injury in IgAN, but not in IgAVN, pointing to disease-specific patterns of complement engagement.
This retrospective biopsy study examined how complement C3 colocalizes with IgA and IgG within glomerular immune-complex deposits in IgA nephropathy (IgAN) and IgA vasculitis with nephritis (IgAVN). Greater C3–IgA colocalization is significantly associated with individual features of active glomerular injury in IgAN, but not in IgAVN, pointing to disease-specific patterns of complement engagement.
Across both conditions, higher composite activity by Oxford M+E+C scores tended to track with stronger pairwise colocalization; these correlations reached significance for C3–IgA in both IgAN and IgAVN, and for C3–IgG in IgAVN.
The findings suggest common yet distinct deposit architectures between the two diseases and support a disease-inducing role for C3–IgA–containing immune complexes, reinforcing complement as a mechanistic and potentially therapeutic axis in IgA-mediated kidney injury.
Randomized, double-blind, placebo-controlled phase 2a study assessing the efficacy and safety of felzartamab for IgA nephropathy
 This phase 2a randomized, double-blind, placebo-controlled study evaluated felzartamab, a fully human anti-CD38 monoclonal antibody, in 54 patients with biopsy-proven IgA nephropathy.
This phase 2a randomized, double-blind, placebo-controlled study evaluated felzartamab, a fully human anti-CD38 monoclonal antibody, in 54 patients with biopsy-proven IgA nephropathy.
By depleting CD38+ plasma cells, felzartamab aims to reduce galactose-deficient IgA1 and autoantibodies, targeting the first and second “hits” in IgAN pathogenesis. Three dosing regimens (2, 5, or 9 infusions over up to 5 months) all reduced proteinuria at 9 months, with the 9-dose schedule achieving the greatest reduction (≈45%), sustained at 24 months.
These findings support felzartamab as a promising candidate that warrants confirmation in larger phase 3 trials.
B cell-derived exosomal miR-483-5p and its potential role in promoting kidney function loss in IgA nephropathy
 Pawluczyk et al. identify exosomal miR-483-5p, predominantly derived from CD19+ B cells, as enriched in the serum of IgAN patients with higher proteinuria who later developed kidney failure.
Pawluczyk et al. identify exosomal miR-483-5p, predominantly derived from CD19+ B cells, as enriched in the serum of IgAN patients with higher proteinuria who later developed kidney failure.
Mechanistically, B-cell exosomes loaded with miR-483-5p induced a pro-inflammatory phenotype in human collecting-duct epithelial cells, likely via SOCS3 suppression; miR-483-5p–enriched exosomes were also detectable in urine.
Clinically, the work highlights a plausible biomarker that integrates B-cell activity with tubular injury pathways, complementing traditional risk markers (proteinuria, estimated glomerular filtration rate decline). If validated longitudinally with standardized sampling and incremental discrimination analyses, miR-483-5p could refine risk stratification and inform biomarker-guided evaluation of B-cell–targeted therapies in IgAN.
KIDNEY INTERNATIONAL REPORTS ARTICLES |
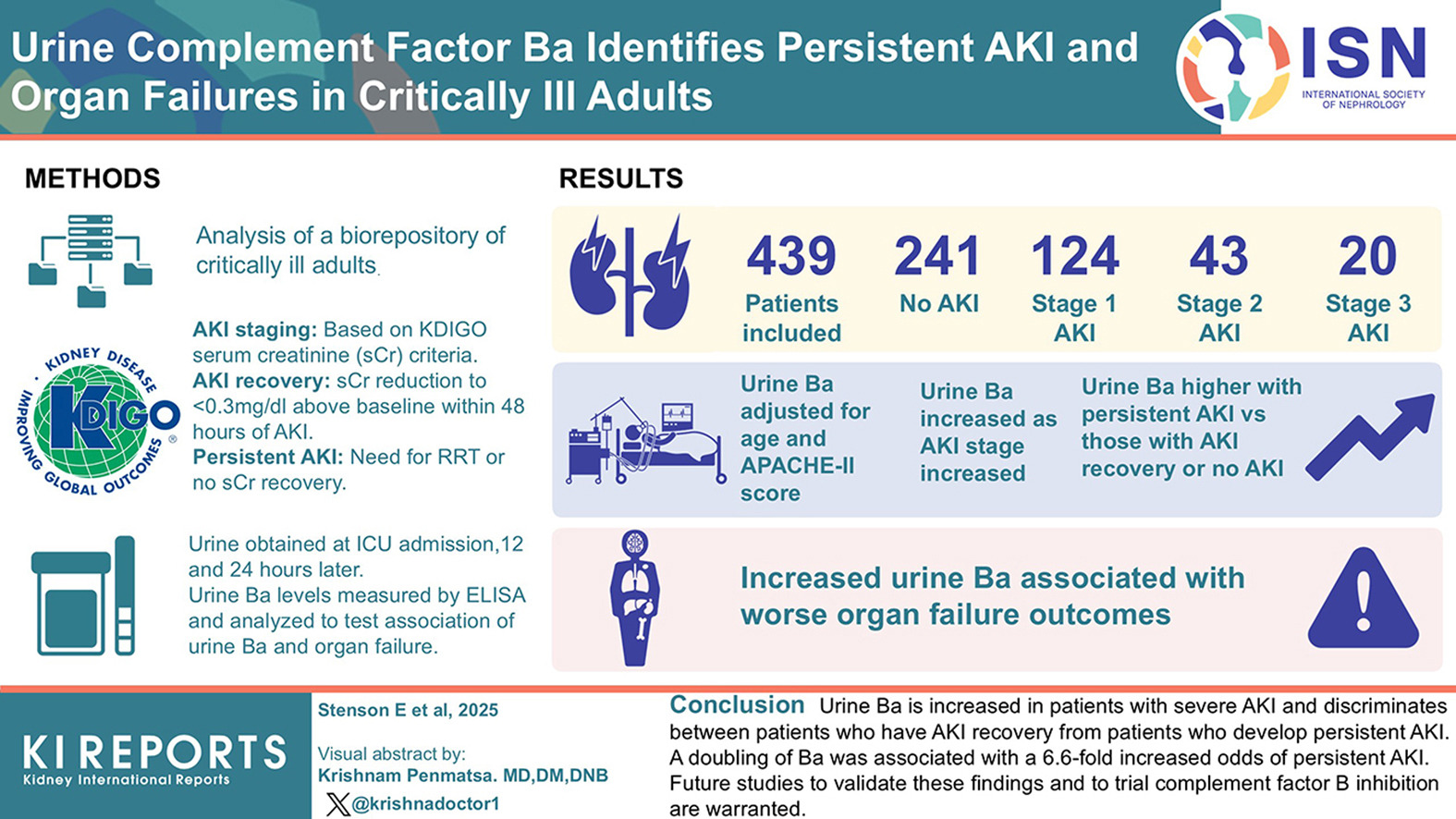
In a cohort of 439 critically ill adults stratified by KDIGO stage (no acute kidney injury [AKI], stage 1–3), higher urinary Ba–a marker of alternative pathway activation tracked with AKI severity–distinguished persistent AKI from recovery.
After adjustment for confounders, an increase in Ba was associated with a ~6.6-fold higher risk of persistent AKI, indentifyingg Ba as a biologically plausible, clinically actionable signal early in the course of treatment in the intensive care unit (ICU)
Patients with higher levels of Ba had worse organ failure outcomes, indicating that complement activation is associated with broader organ failure trajectories. These data position urinary Ba as a biomarker and monitoring tool for trials, especially those testing the proximal alternative-pathway blockade (e.g., factor B inhibitors), while reinforcing the need for prospective validation and assay standardization.
![]()
In kidney ptransplant patients, recurrent IgAN in the allograft was more frequent and linked to significantly worse long-term graft survival compared to de novo IgAN. Recurrent IgAN often presents early post-transplant in the form of mesangial IgA deposition, active proliferative changes, proteinuria, and progressive graft decline.
Prior IgAN in these patients warrants vigilant follow-up, regular urinalysis, early biopsy for unexplained proteinuria, and thoughtful optimization of immunosuppression plus renin–angiotensin system blockade, especially in younger recipients or those with aggressive native disease. Researchers note that research into mechanisms and targeted therapies remains a priority.
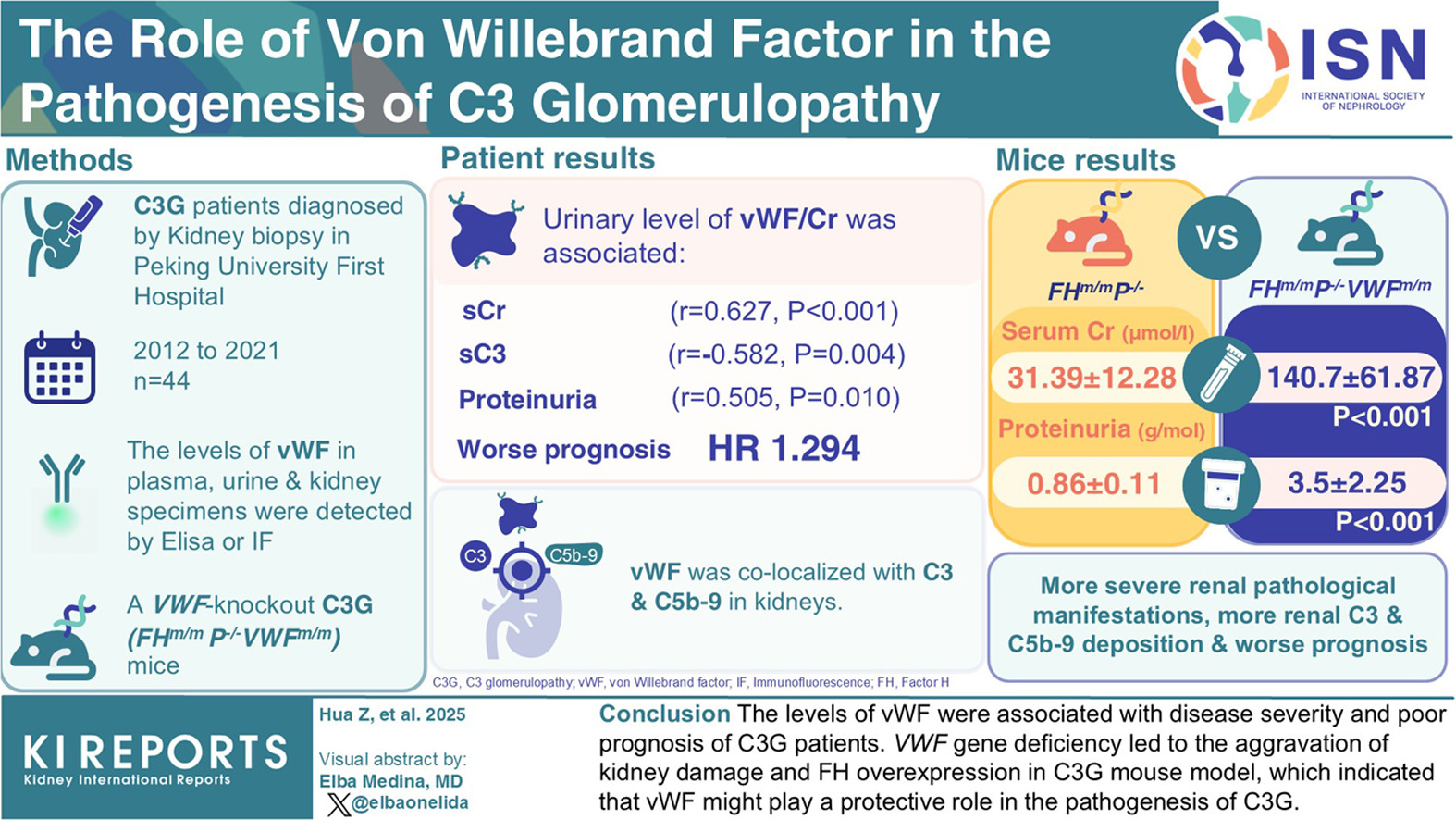
C3 glomerulopathy is driven by dysregulated alternative pathway activity with glomerular C3 deposition. Emerging evidence implicates von Willebrand factor (VWF), an endothelial and platelet-derived hemostatic protein, in modulating this process. VWF may interface with complement regulation and promote intraglomerular thrombus formation, potentially amplifying injury and accelerating kidney dysfunction.
This hemostasis–complement crosstalk opens therapeutic avenues: Targeting VWF–platelet interactions or VWF-linked complement amplification could complement current strategies focused on the alternative pathway. However, mechanistic pathways remain to be fully delineated, and clinical translation will require robust biomarkers and trials that clarify when, and for whom, VWF-directed therapies add value.
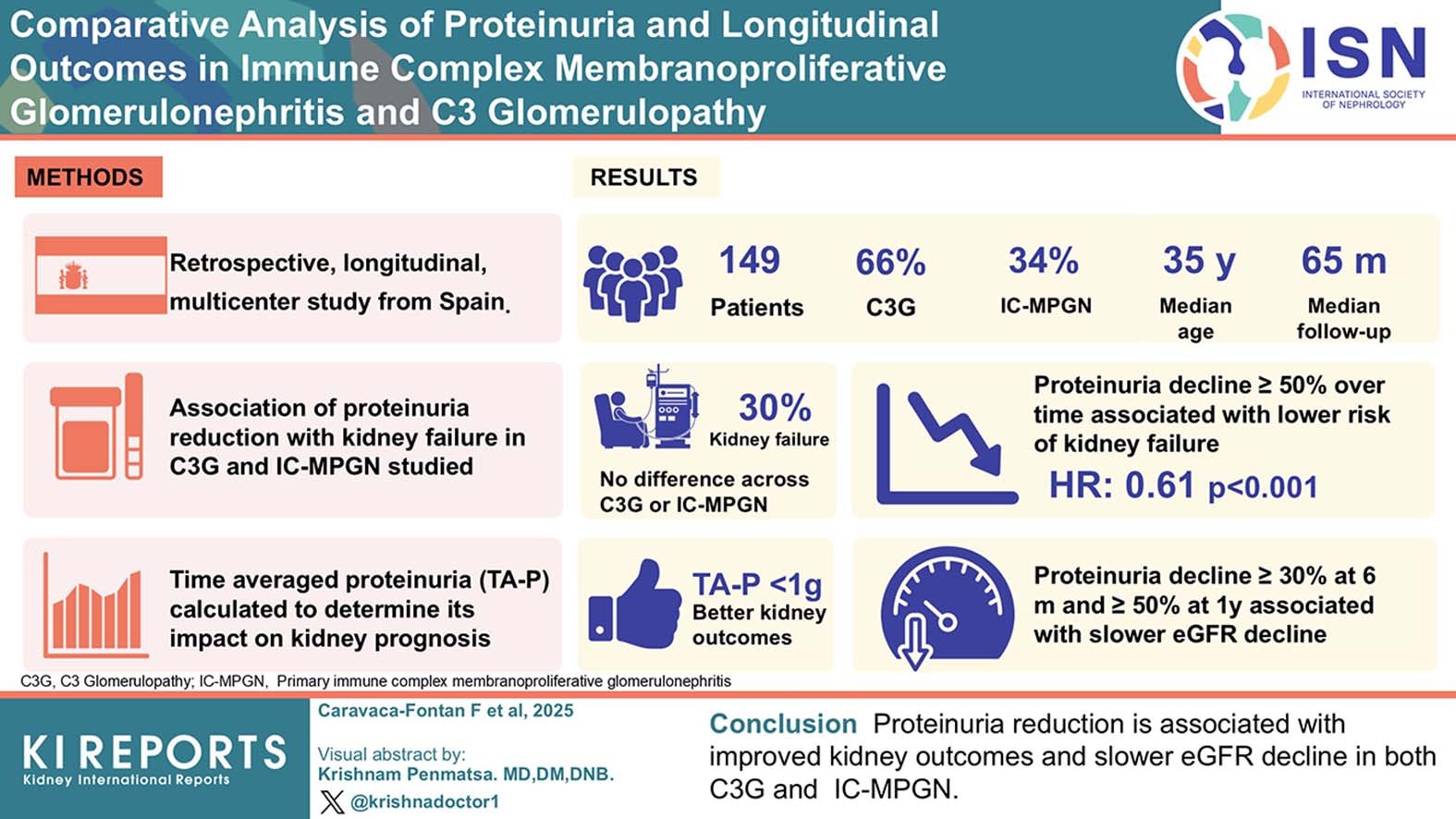
A ≥50% reduction in proteinuria was associated with slower estimated glomerular filtration rate decline and lower risk of kidney failure, whereas rising proteinuria independently predicted adverse outcomes, underscoring proteinuria as a dynamic prognostic biomarker.
The results suggest prioritizing sustained proteinuria reduction and serial monitoring, aiming for a ≥50% decline through immunomodulation, complement-targeted therapy where appropriate, with early escalation if proteinuria rises.
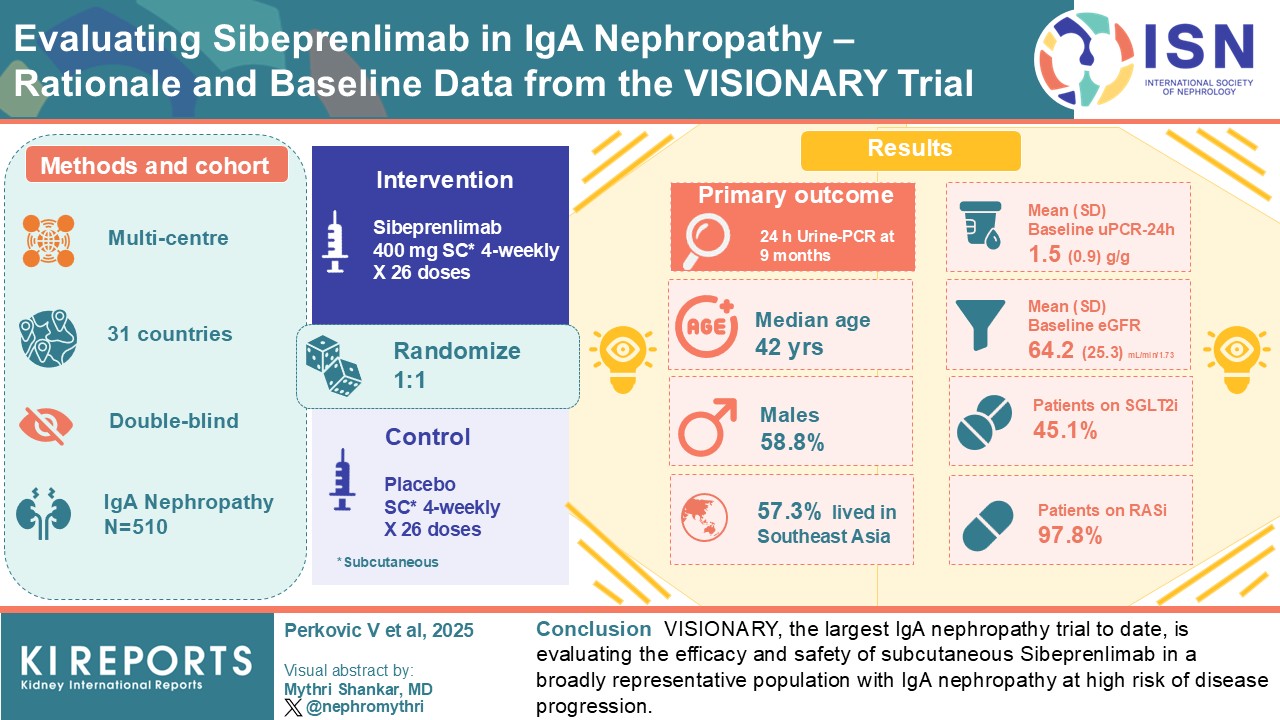
The VISIONARY trial is a large, multicenter, double-blind, placebo-controlled study evaluating sibeprenlimab, a selective A Proliferation-Inducing Ligand (APRIL) inhibitor that lowers pathogenic galactose-deficient IgA1 and immune complex formation in IgA nephropathy (IgAN).
A total of 510 adults with biopsy-confirmed IgAN were randomized 1:1 to subcutaneous sibeprenlimab 400 mg or placebo every 4 weeks for 26 doses, with a change in 24-hour urine protein-to-creatinine ratio (uPCR) at 9 months as the primary endpoint.
Participants (median age 42 years) had a mean baseline uPCR of 1.54 g/g and an estimated glomerular filtration rate of 64.2 mL/min/1.73 m²; almost all were on renin-angiotensin system blockade, and nearly half were on sodium-glucose cotransporter 2 inhibitors.
This global, high-risk cohort and sample size make VISIONARY the largest IgAN trial to date and an important test of APRIL blockade as a disease-modifying strategy.