
December 2025 Edition

Impact Factor 2024
Advancing pediatric kidney care: New insights in ISN Journals
From cystic kidney disease genetics to cardiovascular risk in pediatric dialysis and measuring life participation, pediatric kidney care research is rapidly evolving. This selection of recent papers from Kidney International® and Kidney International Reports® highlights the science and strategies driving more precise, preventive, and equitable kidney care for children.

KIDNEY INTERNATIONAL ARTICLES |
Disruption of the human cystin-1 myristoyl-electrostatic switch causes polycystic kidney disease that phenocopies autosomal recessive polycystic kidney disease
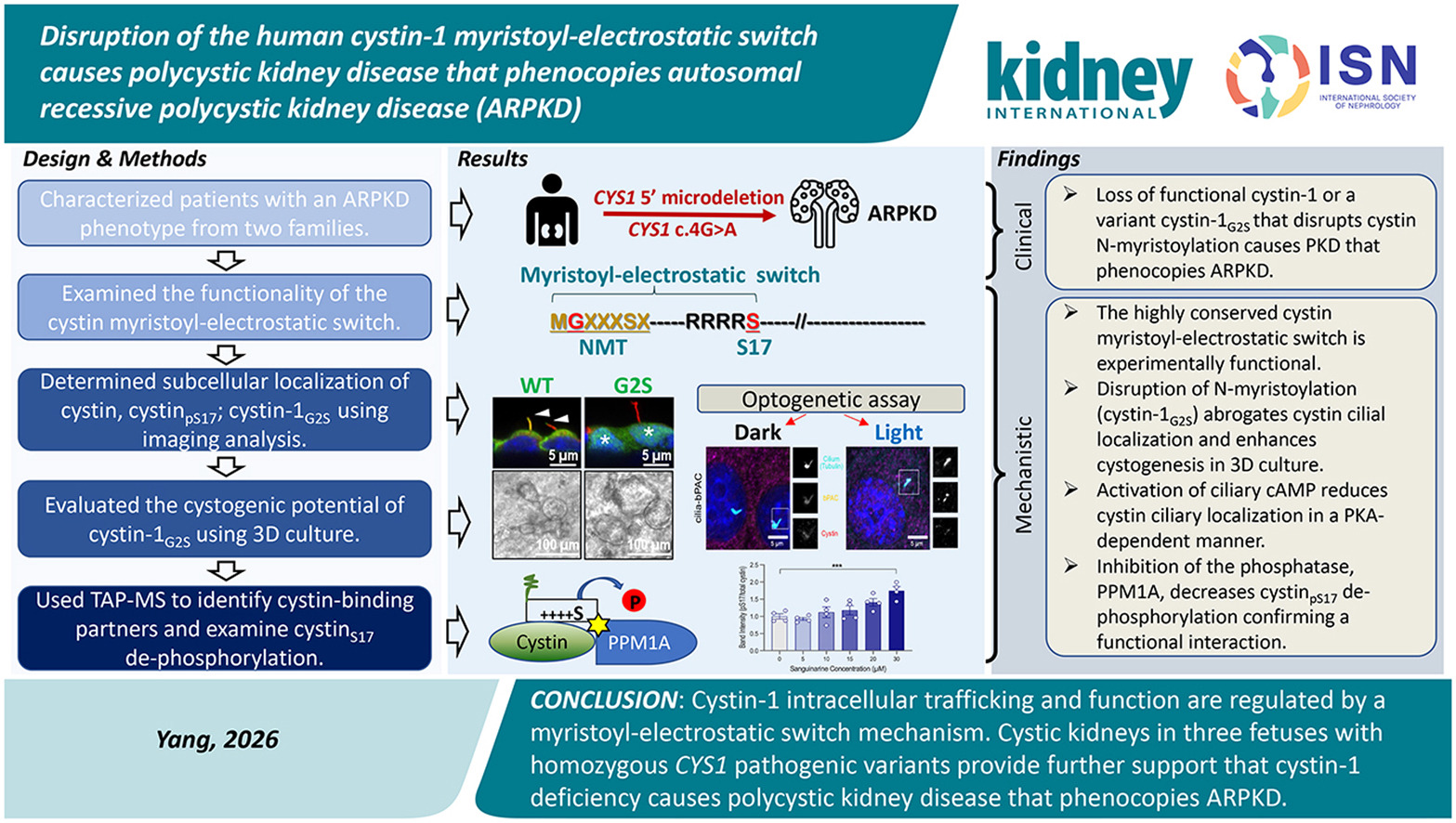
Yang and colleagues describe two unrelated families with enlarged, cystic kidneys consistent with autosomal recessive polycystic kidney disease (ARPKD).
Genetic analyses identified homozygous pathogenic variants in CYS1, expanding evidence that cystin-1 deficiency contributes to fibrocystic kidney disease and underscoring the importance of cystin for appropriate ciliary localization.
Using CRISPR/Cas9 models and 3D culture systems, the authors show that loss of cystin or disruption of its N-myristoylation promotes cystogenesis. Mechanistically, cystin trafficking appears to be governed by a myristoyl–electrostatic switch, with serine-17 phosphorylation downstream of ciliary cAMP–PKA signaling reducing membrane association and favoring cyst growth.
Collectively, these findings position CYS1 as an important ARPKD gene and provide a mechanistic link between cAMP signaling, ciliary protein trafficking, and cyst formation.
Optimizing cardiovascular outcomes in pediatric dialysis
Cardiovascular disease is the major determinant of long-term outcomes in children receiving dialysis. This review emphasizes that the injury trajectory begins well before dialysis and then accelerates during kidney replacement therapy. The burden reflects a mix of traditional risks (hypertension, dyslipidemia, insulin resistance) and kidney-specific drivers (volume overload, chronic inflammation, anemia, CKD–mineral bone disorder, endothelial dysfunction, and uremic toxin exposure). In practice, cardiovascular risk in pediatric dialysis is cumulative and multifactorial, not a late complication that appears only after years of treatment.
A key contribution of the review is its focus on treatment-related factors. Conventional dialysis schedules may leave children exposed to persistent fluid, pressure, and toxin stress, while peritoneal dialysis and standard hemodialysis carry different cardiovascular trade-offs. More intensive strategies are biologically plausible, but pediatric outcomes evidence remains limited. The clinical takeaway is prevention-first and pathway-based: earlier surveillance, tighter blood pressure and volume control, individualized dialysis prescriptions, and proactive management of metabolic and inflammatory drivers starting in early CKD and continuing through dialysis.
Primary hyperoxaluria(s): From trials to real-life data and pipeline therapies
Primary hyperoxaluria (PH) comprises a group of autosomal recessive disorders that can lead to recurrent kidney stone disease, early kidney failure, systemic oxalosis, and the need for combined liver–kidney transplantation.
In this mini-review, Bacchetta et al. summarize recent advances in PH pathophysiology, diagnostics, and therapeutics, highlighting the transformative role of RNA interference (RNAi), which enables precise, sequence-specific silencing of target mRNA.
Small interfering RNA therapies (lumasiran, nedosiran) offer a targeted, liver-directed strategy to reduce hepatic oxalate production and have shown significant, sustained reductions in urinary oxalate in patients with PH1.
Despite these advances, key challenges remain, including timely diagnosis, longitudinal assessment of systemic oxalate burden, limited long-term outcome data, and equitable global access to high-cost therapies. Emerging approaches such as gene editing, mRNA-based therapies, and oral alternatives may further broaden the treatment landscape and improve accessibility.
SGLT-2 inhibition in pediatric CKD: Advances, challenges, and opportunities
Adult trials demonstrating cardiovascular and renal benefits with SGLT-2 inhibitors have typically relied on traditional chronic kidney disease (CKD) endpoints such as proteinuria/albuminuria and estimated glomerular filtration rate (eGFR). However, pediatric CKD differs from adult disease, with less proteinuria and a higher proportion of congenital and non-glomerular etiologies.
Participants in a 2023 stakeholder workshop highlighted the pressing need for pediatric evidence and noted increasing off-label use of SGLT-2 inhibitors in pediatric care. Child-specific safety concerns include dehydration or volume depletion, infections, and potential impacts on growth, bone health, and neurodevelopment.
Pediatric clinical trials should prioritize age-appropriate, disease-relevant endpoints and consider integrating biomarkers of tubular injury and early cardiovascular morbidity alongside safety indicators such as growth velocity and neurocognitive outcomes. Ongoing studies (e.g., EMPAKIDNEY-Kids, DOUBLE-PROTECT) and observational cohorts of children already receiving SGLT-2 inhibitors will be critical to inform safety and effectiveness. Coordinated international collaboration is needed to close the evidence gap and ensure equitable access to renoprotective therapies for children with CKD.
Establishing a core outcome measure for life participation in children with chronic kidney disease: A Standardized Outcomes in Nephrology — children and adolescents with chronic kidney disease (SONG-Kids) consensus workshops report
The SONG-Kids initiative advances a needed shift in pediatric CKD research: measuring what matters most to children, not only what is easiest to quantify clinically.
In consensus workshops involving 171 participants across 16 countries, a consistent priority emerged — children and families value “life participation,” including the ability to attend school, maintain friendships, and take part in everyday activities, alongside symptom control and survival.
The proposed core outcome measure is notable for its developmental sensitivity and real-world feasibility, using age-appropriate language and flexible interpretation to reflect different contexts and stages of childhood. By centering outcomes defined by children themselves, SONG-Kids provides a roadmap for trials and care models that better capture lived experience and ultimately support children with CKD to thrive, not just survive.
KIDNEY INTERNATIONAL REPORTS ARTICLES |
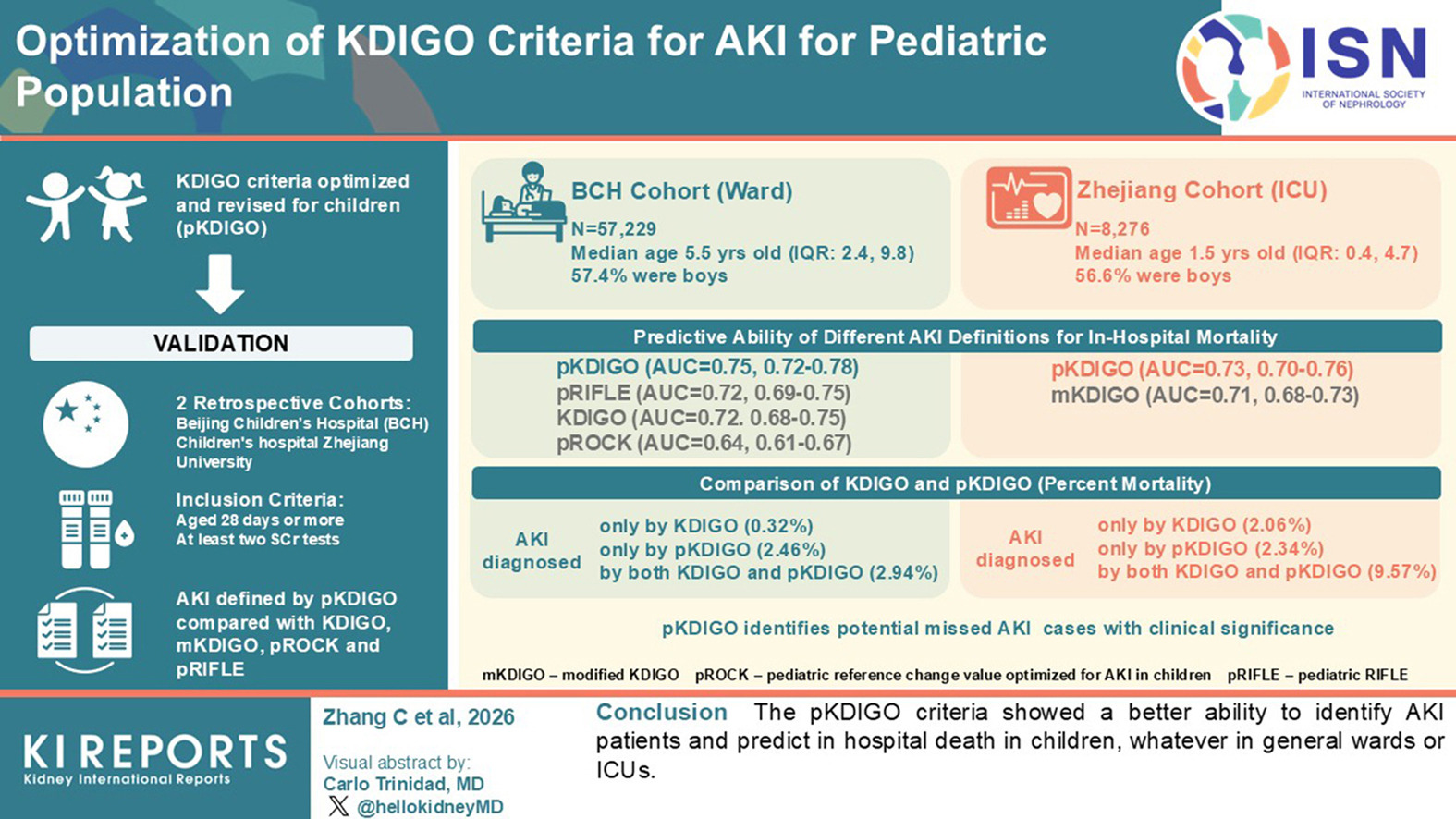
Pediatric acute kidney injury (AKI) definitions still rely largely on adult-derived criteria, applying fixed serum creatinine thresholds despite strong age- and sex-related variation in creatinine biology during childhood. This can cause diagnostic misclassification and reduce prognostic precision in routine pediatric care.
To address this gap, the authors developed a pediatric-adapted Kidney Disease: Improving Global Outcomes framework (pKDIGO) designed to better align diagnostic thresholds with pediatric physiology. They validated pKDIGO in two large retrospective cohorts from China, Beijing Children’s Hospital (n=57,229) and an external Zhejiang PICU cohort (n=8,276), and compared performance against KDIGO, modified KDIGO, pROCK, and pRIFLE, using in-hospital mortality as the primary endpoint.
pKDIGO showed stronger discrimination (AUROC ~0.75 in the Beijing Children’s Hospital cohort), and AKI stage escalation demonstrated a clear dose–response relationship with mortality risk. These findings were directionally replicated in the external PICU cohort.
Overall, pKDIGO appears to be a clinically relevant advance in pediatric AKI phenotyping and risk stratification, with potential to support earlier recognition, improved triage, and more targeted intervention pathways for children at highest risk.
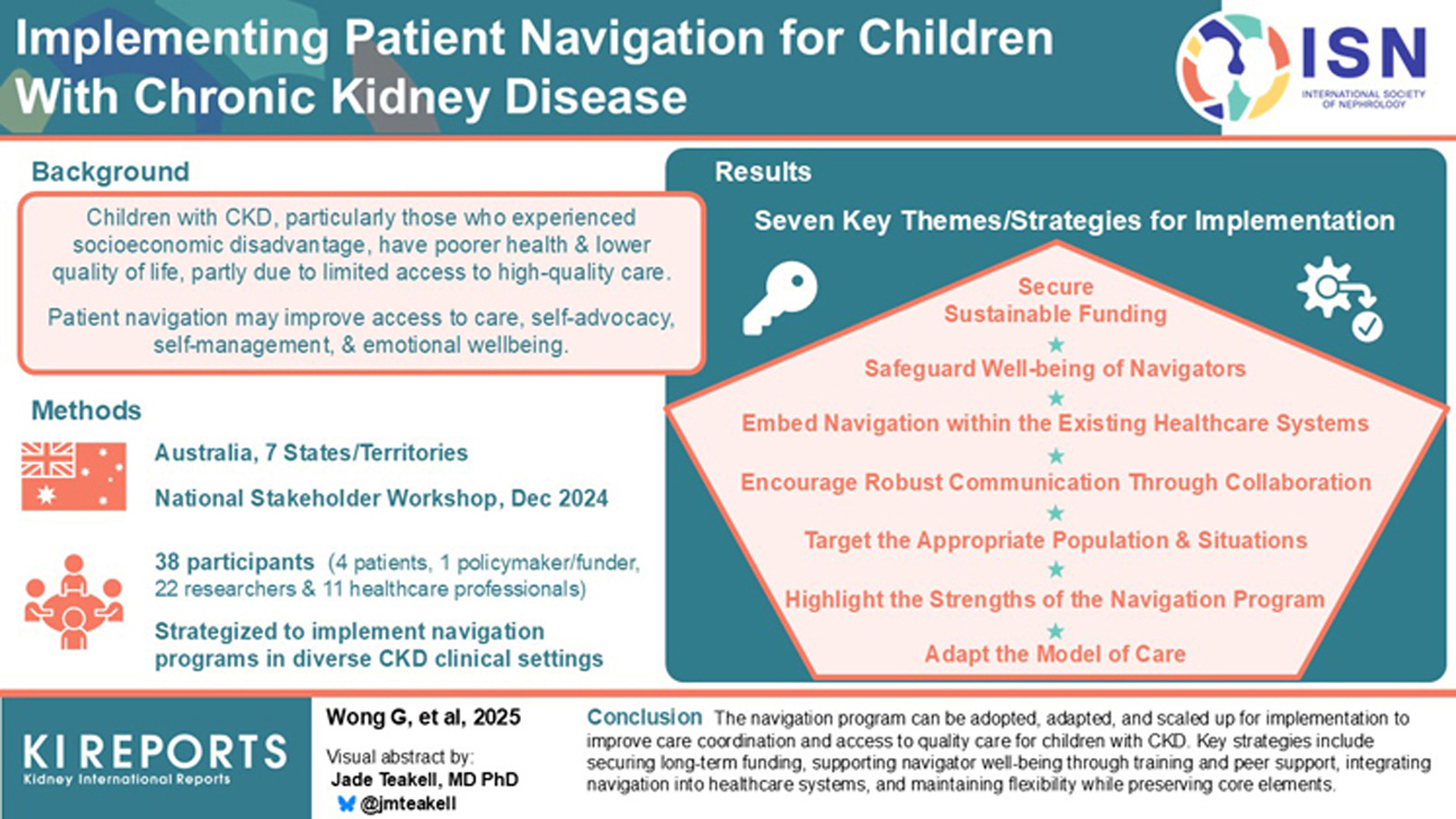
This article on implementing patient navigation for children with chronic kidney disease (CKD) highlights how structured navigation programs can reduce long-standing disparities by improving access to services, strengthening care coordination, and deepening family engagement.
The authors outline seven practical implementation strategies, such as securing sustainable funding, embedding navigators within multidisciplinary teams, supporting navigator well-being, and tailoring support to the needs of the most vulnerable families.
The take-home message is clear: Navigation should not be an “add-on,” but an integrated component of CKD care pathways to reduce fragmentation, strengthen shared decision-making, and promote more equitable outcomes for socioeconomically disadvantaged children.
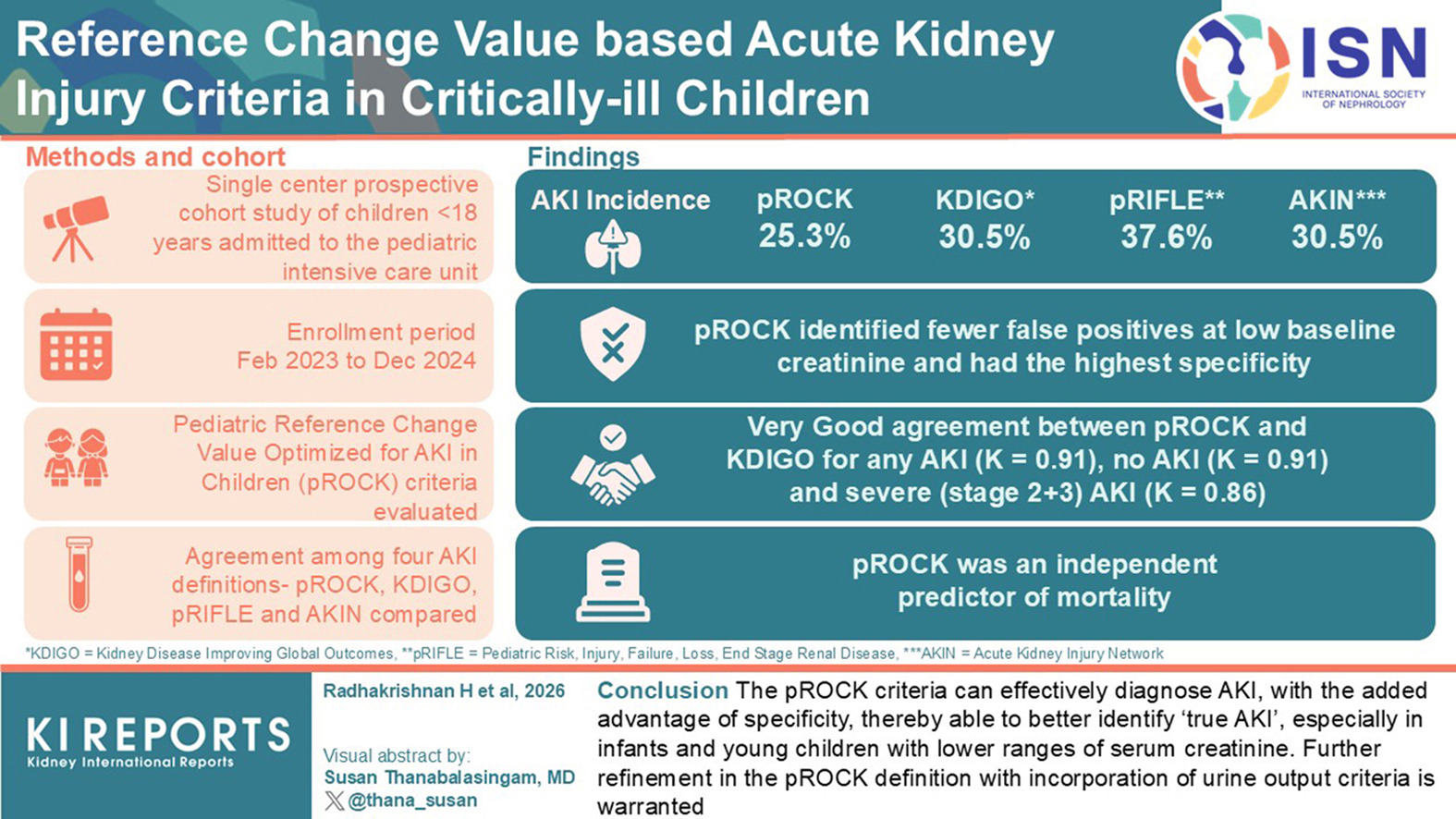
Serum creatinine shows substantial biological and analytical variability in children, making acute kidney injury (AKI) definitions based on small creatinine changes vulnerable to fluctuations.
The pediatric reference change value optimized for AKI (pROCK) is a newer creatinine-based criterion for defining AKI with limited evidence of accuracy. A new study demonstrates its specificity. The authors prospectively enrolled consecutive children aged 1 month to 18 years admitted to a tertiary care pediatric intensive care unit (PICU) between February 2023 and December 2024. AKI within 7 days of PICU admission was assessed using pROCK and compared with conventional AKI criteria.
Of 907 screened patients, 478 were eligible and followed until discharge. Agreement between pROCK and KDIGO was good for stage 3 AKI (kappa = 0.76) and very strong for diagnosing any AKI and no AKI (kappa = 0.91 for both). pROCK had the highest specificity (96.2%), whereas KDIGO had the highest sensitivity (100%). pROCK was an independent predictor of mortality.
Overall, pROCK may improve specificity, particularly in infants and young children with low baseline creatinine; however, further refinement should incorporate urine output requirements.
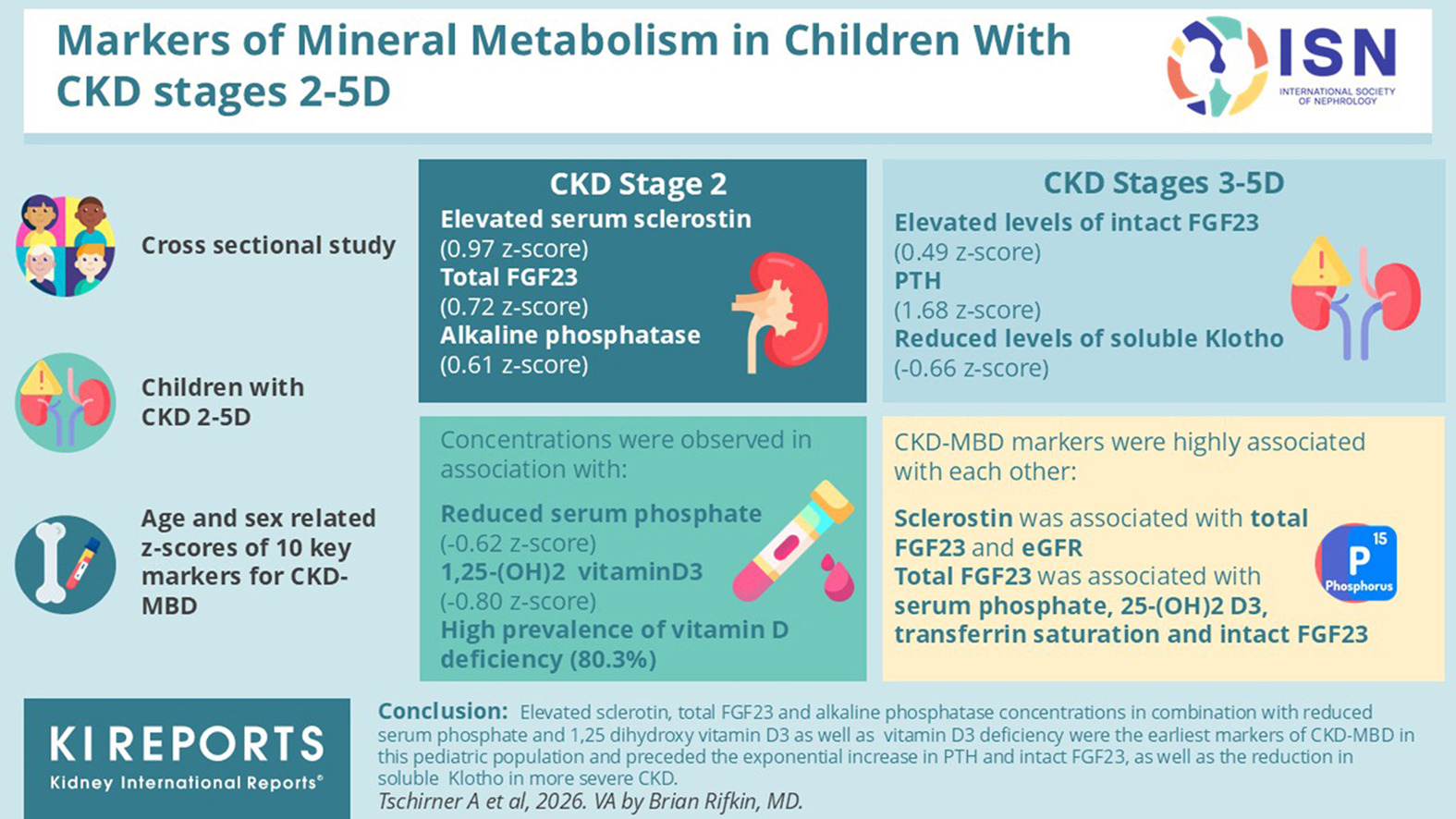
This cross-sectional study of 170 children with chronic kidney disease (CKD) stages 2–5D used age- and sex-adjusted z-scores to characterize early CKD–mineral and bone disorder (CKD-MBD).
Compared with healthy peers, stage 2 already showed higher sclerostin, total FGF23, and alkaline phosphatase, with lower phosphate and vitamin D metabolites, while iPTH, iFGF23, and soluble Klotho were largely unchanged.
With progression, abnormalities intensified: total fibroblast growth factor (23FGF23), alkaline phosphatase, and phosphate rose from stage 3a onward, whereas calcium, 1,25-dihydroxy vitamin D3, and soluble Klotho declined; hyperphosphatemia and hypocalcemia appeared mainly in stages 4–5D.
The pattern suggests FGF23/sclerostin changes precede “classic” derangements, supporting earlier CKD-MBD surveillance during growth and attention to modifiable factors such as vitamin D and iron status.
Using 16S rRNA sequencing, this prospective cohort study compared urinary microbiomes in 36 children with CAKUT (low- vs. high-risk of urinary tract infection [UTI]) and 44 controls. Diversity decreased stepwise from controls to low-risk to high-risk CAKUT, with distinct community clustering and greater inter-individual variability in those at the highest risk, consistent with dysbiosis even before symptomatic infection.
During follow-up, UTI-free survival was lower in the high-risk group, and baseline microbiome profiles tended to be more “control-distant” among children who later developed a UTI. Depletion of health-associated consortia correlated with poorer UTI-free survival, and specific taxa tracked with higher or lower future risk.
These findings support urinary microbiome profiling as a non-invasive tool to refine risk stratification and better target prophylaxis while promoting antimicrobial stewardship.